What are Fibroids?
Fibroids are a non-cancerous growth deriving from smooth muscle in the wall of the uterus (womb). They are present in around a quarter of all women at some time in their lives. Some fibroids are tiny, only a few millimetres across while others may continue to grow and reach a large size. Fibroids are usually harmless and are often undetected. Symptoms are experienced by only around 30% of women with fibroids.
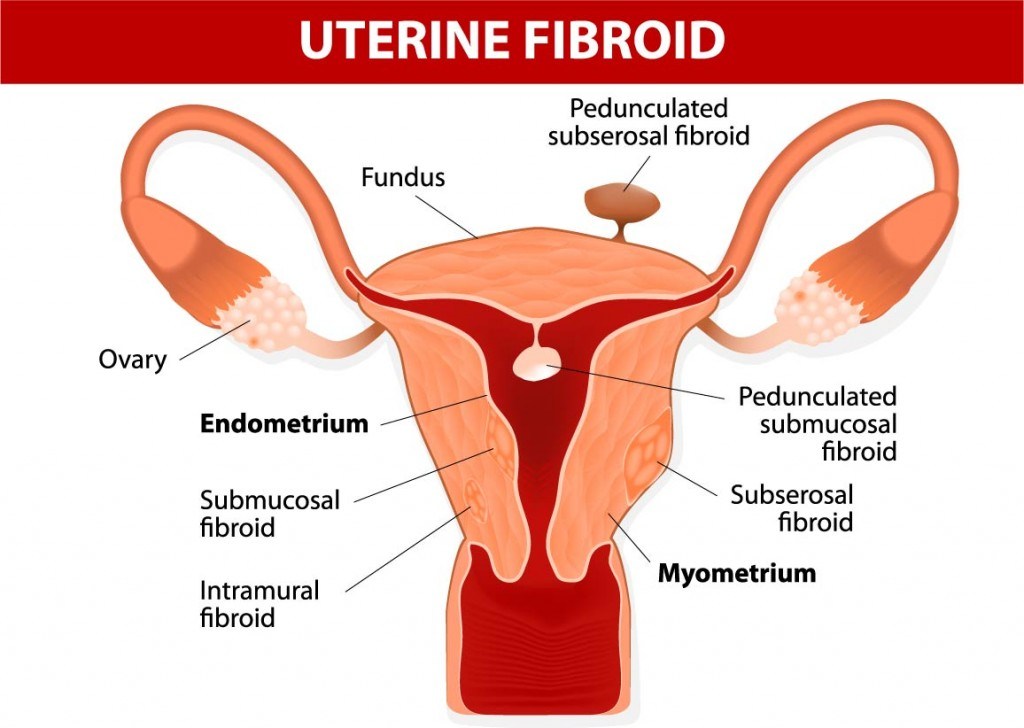
Types of Fibroids
Fibroids are named according to their location as follows:-
Intramural fibroids are the most common type of fibroid and grow within the muscle tissue of the womb, beginning as small nodules which may cause distortion to the uterine cavity as they grow.
Subserosal fibroids grow from the outside wall of the uterus into the pelvis and can sometimes become very large. Occasionally they can be attached to the uterus by a stalk in which case they are known as pedunculated fibroids. When subserosal fibroids become very large, they may press on the bladder or other pelvic organs and become symptomatic.
Submucosal fibroids grow from muscle beneath the endometrium of the uterus and may distort the uterine cavity. A pedunculated lesion within the cavity is called an intracavitary fibroid. Even small submucosal fibroids may lead to bleeding or fertility problems because they originate just under the endometrium, which is the inner lining of the womb. They are not very common, only accounting for around 5% of cases.
What Causes Fibroids?
It is not completely clear why fibroids develop in some women, there may be a genetic component as they are slightly more common in afro-carribean women. Also women with obesity, polycystic ovary syndrome, diabetes and hypertension are slightly more likely to develop fibroids. Fibroids are sensitive to the female hormone estrogen and grow more quickly in situations where estrogen levels are high, for example during pregnancy. They also shrink after the menopause as estrogen levels decline.
Problems and Symptoms Related to Fibroids
Fibroids are usually harmless and often undetected. Symptoms only occur in about a third of women who have fibroids. The menstrual cycle is not affected by fibroids, but sometimes bleeding can be heavier or more painful than normal. In the case of very large fibroids a bloating or swelling in the abdomen can occur. Large fibroids pressing on the bladder or bowel may cause constipation or the urge to urinate more frequently. If fibroids are located close to the cervix they may cause pain during sexual intercourse.
Fibroids and Fertility
Only a very small proportion of fibroids are likely to affect fertility, probably less than 5% of them. There is still considerable scientific research and debate on this subject. It is likely that subserosal fibroids have little or no effect, whereas submucosal fibroids are more likely to have an effect because of their position just under the lining of womb. It has been suggested that large intramural fibroids may in some cases alter the blood flow to the uterine lining as well as altering the shape of the uterine cavity. There can be considerable variation in the presentation of fibroids however, and whatever the type, there are four main ways in which fertility might be affected. Firstly, excessive fibroid growth may affect the blood supply to the endometrium reducing its receptivity to the embryo. Secondly, the uterus may become slightly enlarged or distorted by the presence of a fibroid and a cavity with an abnormal contour could prevent normal implantation. Thirdly, distortion of the cervix or uterus might prevent effective progress of sperm. Finally, segments of the fallopian tubes could be obstructed by the fibroid, preventing effective fertilisation of the egg and subsequent transport of the resulting embryo.
Fibroids and Pregnancy
Given that fibroids are so common and usually do not interfere with fertility, many women with fibroids become pregnant. During pregnancy there is an increase in female hormones which often causes fibroids to grow more quickly. In most cases, this doesn’t affect the pregnancy or cause any symptoms. In a few cases however, fibroids can create a slightly higher risk of miscarriage or premature labour. If the fibroids grow in such a way that they obstruct the birth canal, they may increase the difficulty of labour or cause the baby to be in the incorrect position requiring caesarean section. Fibroids are not normally treated during pregnancy.
Diagnosis of Fibroids
Ultrasound
Some fibroids can be felt as lumps during a pelvic examination, but the gold standard for detecting them is ultrasound scan. Ultrasound is completely harmless and painless in that it only uses high frequency sound waves to image the uterus and ovaries. It may be carried out transabominally where the ultrasound probe is moved over the abdomen; or transvaginally where the probe is introduced into the vagina. A variation of the technique uses ultrasound along with salt water with which the uterine cavity is filled before the ultrasound examination. This technique is called hysterosonography and gives a very detailed picture of the surface of the wombs lining.
Hysteroscopy
Hysteroscopy provides a means of directly observing the inside of the uterus and can therefore detect the presence of fibroids, polyps, or other causes of bleeding. A long flexible or tube called a hysteroscope is introduced through the cervix to reach into the uterus. A fibre optic light source and camera in the tube allow the doctor to view the cavity. A similar technique can be used to surgically remove fibroids. In a few cases the surgeon may take an endometrial biopsy to rule out the possibility of malignancy.
Laparoscopy
Laparoscopic surgery may be performed to diagnose fibroids. This involves making small incision made near the navel and viewing the inside of the pelvis laparoscope. Of course in this case the outside of the uterus is being viewed, including the fallopian tubes and ovaries.
Fertility and Treatment of Fibroids
Of course all fibroid problems can be completely eliminated by hysterectomy (removal of the womb) and this has been the classical treatment where fibroids are causing symptoms and fertility is not an issue. Alternatively milder symptoms such as heavy bleeding have been treated with pharmaceutical agents similar to contraceptives or with intrauterine coils. Of course neither of these approaches are options in the woman trying for a baby.
Some medical research has suggested removal when fibroids measure over 5 centimetres in diameter and are located within the uterine wall (intramural). Each situation is different and the advice of an experienced fertility consultant should be sought. If the uterine cavity is normal, the fibroids are small, or located on the surface of the uterus patients are often advised to have a repeat ultrasound scan to assess whether the fibroids are growing. In most cases, fibroids do not cause symptoms and are not considered a threat to fertility or pregnancy and no treatment is necessary. In situations where fertility is being affected there are several methods that may be employed depending upon the situation.
Myomectomy
The first of these is surgical removal, called myomectomy. This can be done via an abdominal incision of the bikini type, usually performed when the fibroids are large or very numerous. Alternatively a laparoscopic approach, so called keyhole surgery can be employed. This is less invasive and usually used where fibroids are small. Fibroids that are mainly inside the uterine cavity are removed hysterocopically. This is where an operative instrument called a hysteroscope is inserted via the cervix and the fibroids removed. The type of operation depends on the size, number and position of the fibroids. There is a small risk of very heavy bleeding with this operation and in some cases a hysterectomy may be needed if that situation occurred. Myomectomy is generally a safe procedure with few postoperative complications, but fibroids removed in this way often grow back again later.
Uterine Artery Embolisation
A more recent treatment for removing fibroids whilst preserving fertility is uterine artery embolisation (UAE). This involves introducing a thin flexible tube called a catheter into blood vessel in the leg and guiding it to an artery that supplies the fibroid in the womb. This is achieved using X-ray guidance to monitor the progress of the catheter. Once in-situ, a substance that blocks the artery is injected through the catheter. This deprives the fibroid of its blood supply causing it to shrink. It usually takes 6-9 months for the fibroid to regress fully. There is currently a lot of medical interest in UAE and it is the least invasive of all techniques as far as the uterus is concerned. There is not yet enough data comparing UAE with myomectomy in a fertility context, but this question is currently the subject of research.
Ablation and Ultrasound
Fibroids that are close to the inner lining of the womb may be treated by ablation them using lasers, microwaves or a heated wire loop. In addition, pulses of high powered ultrasound can targeted at the fibroid under Magnetic Resonance Imaging (MRI) guidance. Any of these techniques may be appropriate in a specific situation as advised by the consultant, but there is currently not enough evidence to dictate their widespread use.
Summary
Fibroids alone cause infertility in a very few women, probably less than 3%. However, they may be contributory factor in impaired fertility and also increase obstetric risk. Your fertility consultant will generally seek to rule out other causes of infertility before recommending treatment for fibroids. If you are one of the women in which fibroids are the major factor, then there are several diagnostic and treatment options open to you.
Science Director Concept Fertility Clinic www.conceptfertility.com